Path to diagnosis (Part I: An empty sella)
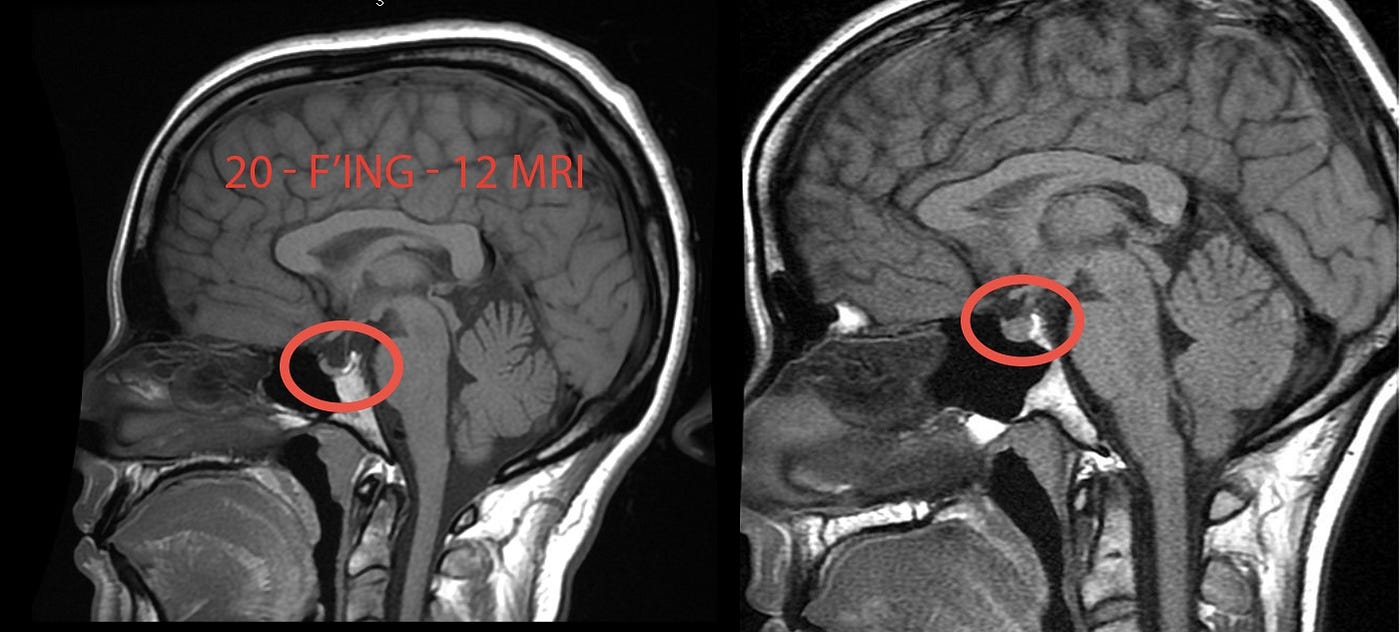
My path to a craniocervical instability (CCI) diagnosis began when a vascular neurosurgeon emailed me to say, “some of my Ehlers-Danlos Syndrome* patients develop exactly your symptoms after a severe viral infection.” He reached out because he had seen my brain MRI while watching Unrest. I had included it as an artistic choice, and he noticed that my supposedly normal MRI was in fact not normal. I had an empty sella — a finding he considered significant — and he offered to take a look at my original imaging.
An empty sella is when the sella, a bony space which holds the pituitary gland, appears “empty” (dark/black) on an MRI. This is because the space has been filled with cerebrospinal fluid, flattening the pituitary gland. Most radiologists and neurologists will consider this an “incidental finding,” meaning they believe it’s irrelevant to your symptoms. In my case, as so often happens, the radiologist didn’t even include it in the report. (This is why it is important to always request your original imaging discs, not just the report.)
In reality, it is only an incidental finding if the patient does not also have the symptoms of intracranial hypertension: elevated pressure in the head. As it turns out, I did have symptoms, namely headaches and a feeling of pressure in my head and behind my eyes. This rise in pressure can be due to excess cerebrospinal fluid, excess blood or in some cases, excess brain (e.g., brain swelling). With symptoms, empty sella is considered a sign of intracranial hypertension.
This neurosurgeon (who again, is not the neurosurgeon who ultimately operated on me — his is a different specialty) treats a wide range of the usual vascular neurological conditions like stroke or aneurysm. He has also developed a sub-specialty treating intracranial hypertension in patients with Ehlers-Danlos Syndrome.
The neurosurgeon looked at my original 2012 MRI and confirmed that yes, I had an empty sella and that I also had excess cerebrospinal fluid in my optic nerve sheath, a second sign of intracranical hypertension. There is a scene in Unrest, after I come back from my college reunion, where I collapse on the front porch, screaming. I say, “I could feel my head, swelling, pushing out my eyeballs.” Turns out, that is what it feels like to have spinal fluid behind your eyes.
He further explained that in patients with high intracranial pressure, the spinal fluid needs somewhere to go. So the fluid will fill the sella, crushing the pituitary gland, and fill the optic nerve sheath. He said that while these findings were consistent with intracranial hypertension, to confirm the diagnosis, I would first need to do an MR venogram (an MRI that uses contrast to visualize the veins) and a high volume lumbar puncture.
So in March 2018, after all the travel for Unrest had died down, I had an MRV. It confirmed the empty sella and the excess optic nerve sheath fluid he had seen on my 2012 MRI. It also confirmed that I had bilateral transverse venous sinus stenosis (TSS), a narrowing of two veins in the back of the head that drain blood from the brain. TSS is found in 83% of cases of intracranial hypertension (compared to 3% of controls). (It is not known whether TSS is cause or effect, but there is growing evidence that stenting one of the transverse sinus veins can resolve intracranial hypertension.)
One purpose of the high volume lumbar puncture was to see whether temporarily reducing spinal fluid volume in my brain, and thus lowering my pressure, would result in any changes in my symptoms. It wasn’t a sky-opening miracle but several symptoms did improve. Notably, I could read again! (It was through this experience that I learned that my inability to read long-form was my eyes getting tired moving left to right across the page due to the constant pressure behind them.) My head felt clearer. I could also turn circles in my wheelchair and be in a car going in reverse without becoming dizzy or confused, something that had been a major problem since the beginning of my illness. A picture was emerging, based on both objective and subjective evidence, that I indeed had intracranial hypertension.
There was just one snag: my opening pressure (the pressure measured when they insert the needle into your lumbar spine) was only 17 cm H20. The diagnostic criteria for classic intracranial hypertension requires an opening pressure of 20 cm H2O or higher in non-obese patients, 25 cm H2O or more in obese patients. I had the symptoms, the imaging, but not the opening pressure.
My neurosurgeon explained that while some of his EDS patients do have opening pressures out of the normal range, most of them do not but rather fall into a “high normal” range. (Above average, but still technically normal.) He said, “but for some reason, this still causes symptoms and many benefit from treatment.” Treatment, in the case of his patients, generally involves either putting a stent in the collapsed veins (usually the transverse sinuses) to restore normal blood flow or implanting a shunt to drain excess cerebrospinal fluid. (He is not a fan of long-term use of Diamox, a drug that decreases cerebrospinal fluid production. I know some people swear by it.)
OK, by now you may be thinking, “I don’t have EDS, Jen doesn’t have EDS, what does this all have to do with ME?” I’m not sure, but there are clinicians in the United Kingdom who found exactly the same phenomenon among a cohort of CFS patients presenting with pressure headaches. Here is the summary of that research, which I wrote on this MEpedia page (see MEpedia for the original citations):
A case study of a woman presenting with symptoms of CFS and pressure headache, who was diagnosed with borderline intracranial hypertension, found that her CFS symptoms resolved with the placement of a transverse sinus stent.[3] A cross-sectional study of twenty patients presenting at a headache clinic found that a large proportion of patients had borderline intracranial hypertension, with four meeting the diagnostic criteria for IIH (mean cerebrospinal fluid pressure was 19 cm H2O (range 12 — 41 cm H2O); however, none had clinical signs of IIH. Cerebrospinal fluid drainage via lumbar puncture improved symptoms in 17/20 patients.[4] Researchers speculate that a subset of CFS patients may have borderline cases of idiopathic intracranial hypertension without papillodema.[5]
My neurosurgeon said that while my symptoms did improve with the lumbar puncture, he suspected the problem was more likely to be related to blood flow. The next step was to perform an invasive angiogram, a test conducted under twilight anesthesia, where they insert a probe via a vein in your groin and directly measure the pressure in your transverse sinus veins. Yikes.
Meanwhile, my thyroid cancer surgery had been scheduled for June. I put the intracranial hypertension diagnosis on the back burner. Then, as a consequence of the thyriod surgery, as I write about here, I got much, much much, much worse.
I developed two troubling, new symptoms: I would stop breathing every time I laid on the back of my head and would fall over and become non-responsive every time I turned my head to the left. To be clear, these symptoms were not a part of my clinical picture the first seven years of illness and only appeared after my thyroid surgery . In addition, after thyroid surgery, all of my ME and POTS symptoms got much worse.
In the process of trying to find out why all this was happening to me, I went to a few of the top institutions in the country. I went to UCLA (they, unhelpfully, scheduled me for a sleep study and told to come back in three months). I went to Stanford (where they actually found the lack of breathing and non responsiveness concerning and urgent — I got a really wonderful workup but one that yielded no concrete answers).
In the midst of all of this, I remembered the invasive angiogram test. I scheduled the test and flew back to the East Coast. It was the most precise test for detecting abnormal arterial or venous blood flow (better than any kind of standard, static imaging with contrast) because it could directly measure the pressure in my arteries or veins across any areas of narrowing in real time. As my neurosurgeon said many times, a vein can be compressed on imaging (a static picture) but it doesn’t necessarily mean that it’s changed the rate of blood flow (a dynamic process). Yes, I let my doctor run a probe from my groin, through my body cavity, up my neck and into the back of my brain while I was reasonably awake. (After that experience, David Systrom’s invasive cardiopulmonary exercise test doesn’t sound so bad after all…)
The upshot of this test was that I did have a pressure gradient in my transverse sinuses: blood was draining slower than perhaps it should be. However, it wasn’t severe enough to be causing all my symptoms, nor could all of my symptoms be explained by poor venous drainage from the brain. When I turned my head — a move that, since my thyroid surgery, would provoke a worsening symptoms — the pressure gradient rose significantly, but the effect was transient (an observation that would be repeated later, under an entirely different set of circumstances).
My neurosurgeon said that I was a candidate for a stent and explained the risks and benefits. He was clear, though, that it would be unlikely to improve the acute symptoms that had developed since my thyroid surgery.
Rather, my symptoms most likely had a different structural cause, one he did not treat but often saw in his EDS patients. He told me, “I think you have craniocervical instability, Jen.”
Continued in Path to Diagnosis: Part II (Cervical Collar)
Read more CCI + tethered cord series posts
Read this disclaimer. Crucially, surgery carries risks and it’s important to remember that in medicine, the same exact symptoms can have multiple, different causes. We have no idea how prevalent CCI is in our community and there’s been no research into its relationship with ME. We do know that it is more common among patients with EDS.
To learn more about the possible links between intracranial hypertension and ME, read the content and references on the intracranial hypertension MEpedia page.
See also this review article, “The link between idiopathic intracranial hypertension, fibromyalgia, and chronic fatigue syndrome: exploration of a shared pathophysiology.”
*Just to clarify and as I have said many times, this neurosurgeon was talking about his patient, not me. I do not have Ehlers-Danlos Syndrome.
